Collaborating for a Sustainable Future (update)
In August 2025, we wrote an article noting that ITI is doing a wonderful job in promoting initiatives with academic partners and cited UCL’s Medical Checklist project as a case for such collaborations.
Professor Federico Federici and I have continued working together on this project that aims to support doctors and nurses by offering practical, easy-to-use guidance on working with interpreters when caring for patients who speak little or no English.
Drawing upon relevant government guidance, our Medical Checklist project contributes to at least two of the action areas of the NHS, which respectively tackle access and barriers to services, and equity, cultural sensitivity and rights.
We reviewed some key existing guidelines for healthcare professionals working with interpreters, which can be up to 56 pages long, thus making them hard to be of practical use for a workforce already heavily overloaded with appointed consultations and surgeries. We extracted from these guidelines 10 most important aspects that doctors should beware. We refined these checklist points to make them succinct to read and easy to act on. On this basis, we designed a Delphi survey. The survey collects all stakeholders’ views towards these ten checklist points, so as to achieve consensus among them regarding what is most important for healthcare professionals to be aware of when they communicate with their patients via interpreters. Our goal is to finalise the checklist once consensus is reached, and to promote its use in NHS hospitals.
We are pleased to share here the outcome of our Checklist project from its first phase of research work.
Support and promotion from the ITI, the CIoL and the NRPSI were pivotal: we received 90 responses in total to our Phase 1 Delphi survey over a two-month period from June to August 2025. The respondents include healthcare professionals, membership associations, certified medical interpreters, interpreter trainers and interpreting researchers. We applied rigorous academic selection criteria to these raw data and identified 33 valid responses for our analysis.
Checklist
In January 2026, the first version of the Checklist received formal endorsement from the ITI, CIoL, and NRPSI. There was an opportunity to discuss the checklist with junior doctors in a training event organised by St Barts’ Cancer Centre in London. During a 90-minute session on communication and trust in treatment consent consultations, 35 doctors participating in the training engaged with evaluating efficient forms of communication when meeting patients who need to be supported by interpreters.
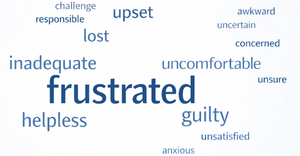
Interacting with patients via an interpreter has both cognitive and emotional impacts on doctors. To set the scene at the training event, we asked the doctors a few informal questions to understand how their experiences of speaking to patients through interpreters made them feel, summarising the responses in one-word answers. From the perspective of studies in medical interpreting, the doctors’ replies were unsurprising, as they showed high levels of uncertainty about interpreter-mediated consultations. The overwhelming majority reported frustration, guilt, inadequacy, and helplessness after interpreter-mediated interactions.

At the training, participants asked several questions along the line of “When can we have this checklist?” and “Can we use it, now?”. In fact, we were able to present the checklist as an A4 document that could be shared with their department or the nurses’ station, stored in their offices (if they had one), saved as a picture on their phones, and so on; 17 laminated copies were taken to share with their departments, and many more as digital photos. The types of emotions mentioned and the participants’ positive reaction to the checklist suggest that the tool could support interpreter-mediated interactions for which doctors are not trained.
Within two days of the event, we received feedback that the checklist could be used more effectively if interpreters were willing to deliver it to doctors during in-person consultations.
Next steps
Phase Two Survey will be available from 20 June. We plan to reach a degree of consensus on any revised wording that may be needed for the card-sized version of the checklist and the finalised larger version.
Version 1.1 is currently available for download – paper copies can be obtained by contacting the authors. As the project follows a Delphi approach, the second phase will optimise the consensus reached and iron out remaining concerns.
Of course, the checklist will never be perfect. However, we know that the cross-sectoral consensus already reached was critical to achieving uptake with the healthcare professionals consulted. A higher degree of consensus is likely to bring on more uptake. With the uptake, the checklist serves a bigger purpose: it reminds us that the conversation about interpreting, patients, and medical trust is much bigger than the narrow narrative that AI can replace high-quality language skills overnight. In our experience, medical professionals already know this, and even when they must make do with technology when professional interpreting is unavailable, they want to find out what works best.